How drugs affect the teenage brain
Before reading this, please refer to the previous blog post to understand the brain terms we will be using, and how drugs affect the brain in general.
There are two important ways in which the teenage brain is uniquely sensitive to and affected by drug use.
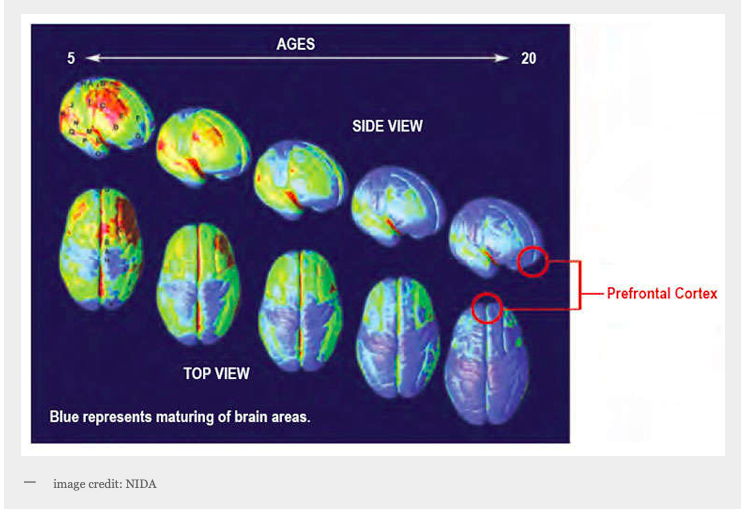
1) During adolescence, the midbrain (the area responsible for reward and motivation, which is profoundly influenced by certain drugs) is well developed, but the prefrontal cortex (the rational part of the brain) is the last area of the brain to develop. As a result, pleasure and emotion—not reasoning—guide most teen behavior.This means teens are more prone than adults to engage in risk-taking behaviors. Their impulses are very powerful, while their ability to control those impulses is not quite as strong.
2) Drugs have an increased impact on the teenage brain, as compared to adults. During adolescence the brain is developing at a rapid rate. Excess grey matter is pruned out, making brain connections more specialized and efficient, which results in a more skilled and well functioning brain. This pruning process is changed by persistent substance use. fMRI machines show altered grey and white matter in the brains of adolescents using substances.
How does this affect the adolescent? Research has shown that certain substances used persistently in adolescence result in a decline in cognitive ability: impaired problem solving; arrested emotional development; difficulty with memory recall; disruptive, chronic, and persistent lack of motivation; increased risk of mental health disorders (other than addiction), including mood disorders, anxiety disorders, and psychotic disorders.
According to research, the earlier an adolescent began using substances, the higher the risk of developing a substance use disorder. Cognitive decline related to substance use is worse for people who started before 18 years old. These cognitive changes persisted even when the adolescent did not use for at least a year
If you are a parent…. DON’T PANIC!
These studies were done on teens with persistent, chronic substance use. The effects of drug use are mitigated by environment, extent of use, and other predisposing factors. Most of us experimented with drugs in our teens, and most of us turned out okay. Not only that, but rates of teen drug use have dropped since the 90s! (Internet addiction has gone up, but that’s a blog post for later….)

Teach your teens about the critical period they are in with respect to their brain development, how this could impact their response to peer pressure and risky situations, and how this makes their brain more vulnerable to the negative long term effects of substances if used persistently. Encourage them to delay substance use as long as possible to reduce their risk of substance use disorders and cognitive deficiencies. Teach them about healthy ways of reducing and coping with stress and peer pressure.
Pay attention to how you lead by example: if you tell your teen to practice healthier ways of coping with stress but then they see you go straight for a glass of wine after a rough day at work…

Well, you see where this is going.
If you are concerned that your teenager may have a problem with substance use already, share your concerns in a calm, open-minded way, and invite them to share any questions or concerns with you. Try to arrange an evaluation by their doctor, who can help determine the extent of the problem and direct you to helpful resources.
Most importantly, when speaking with your teens, keep the conversation neutral and nonjudgemental. Adolescent are curious, and curiosity is important for their developing brain. Share information, rather than just rules, with them. This will help them better understand themselves and their environment, and exercise appropriate caution and sensibility as they develop their independence and explore their world.

 Fowler JS, Volkow ND, Kassed CA, Chang L. Imaging the addicted human brain. Sci Pract Perspect. 2007;3(2):4–16.
Fowler JS, Volkow ND, Kassed CA, Chang L. Imaging the addicted human brain. Sci Pract Perspect. 2007;3(2):4–16.




